
The tide is slowly turning in one of the early fronts of the culture wars, as scientific possibility and questions of personal freedom challenge the assumptions of an earlier generation. Throughout its history, on questions where private vice encounters the desire to create the perfect ‘city on a hill’, the United States has lurched between periods of moral authoritarianism and breezy libertarianism. Prohibition was followed by the era of the three-martini lunch. The most recent of these moral panics – and the most global in its ramifications – was what Richard Nixon chose in 1971 to call “the War on Drugs”. Presented as a public health crisis, it was an opportunity for traditional America to assert its values over what was presented as an un-American, unwashed, morally degenerate opposition that had coalesced around the questions of Civil Rights and opposition to the Vietnam war. The extent of America’s hegemony was such that her allies swiftly fell into line, if they were not compliant already.
In recent years, questions have increasingly been raised as to whether the ‘war’ is winnable at all, let alone worth the immense cost. Recreational drugs remain freely available, untaxed and unregulated as to quality. Drug mafias exert a sinister dominance of civil society in many producing countries, and millions are incarcerated. Famously, one in five black Americans has spent time behind bars because of drug laws.
A less obvious consequence of the criminalisation and stigmatisation of cannabis use was that most scientific research into the plant and its derivatives halted 50 years ago. In the ensuing years, other areas of medical science have made remarkable strides forward. Cannabis, by contrast, is only just beginning to give tantalising glimpses of its potential. There was a good reason this particular narcotic was scientifically interesting, as we shall see.
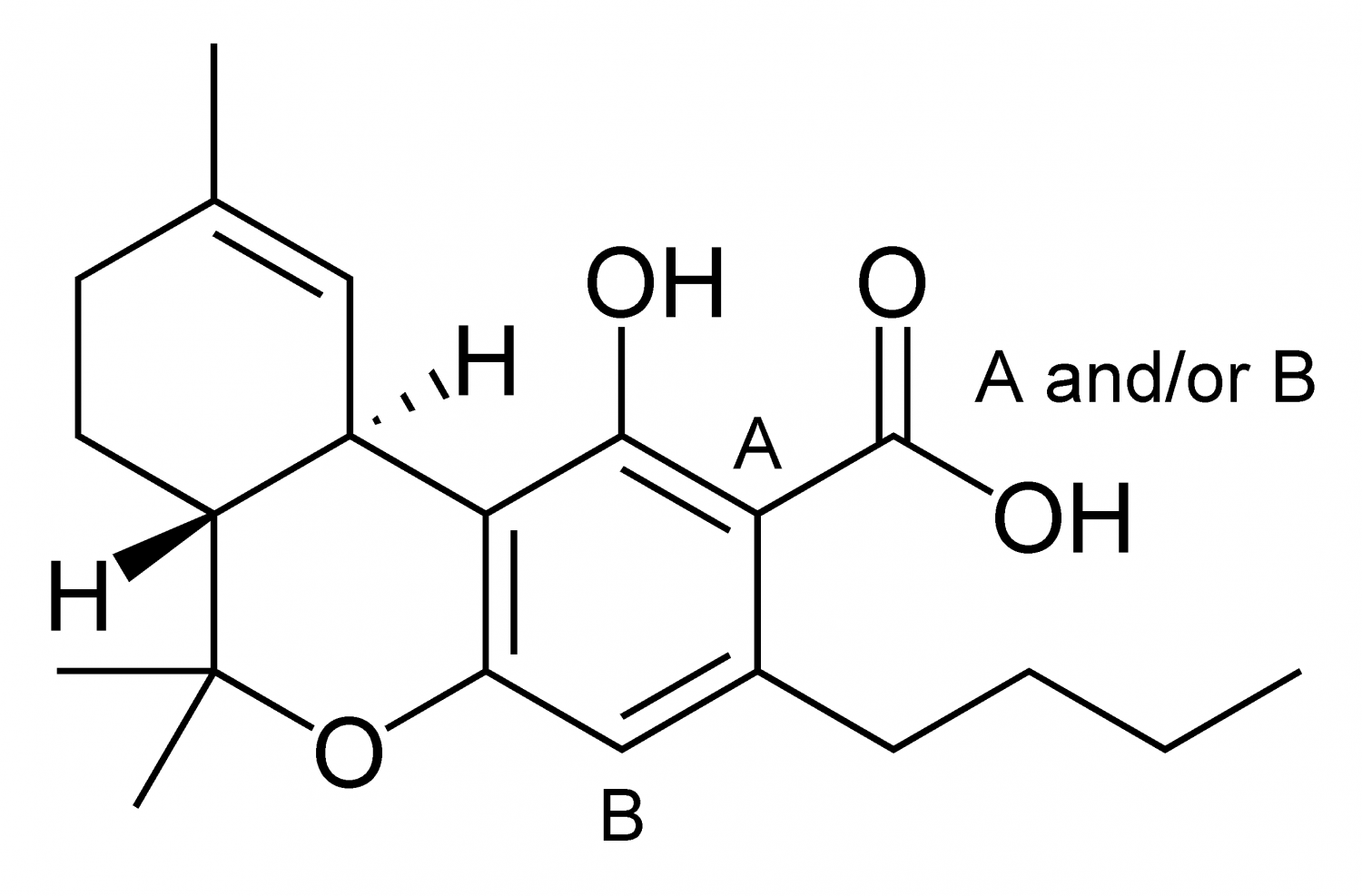
Cannabis is a naturally occurring plant that produces over 100 active ingredients known as cannabinoids. The best known of these are cannabidiol (CBD), a non-psychoactive compound widely sold in health stores, and tetrahydrocannabinol (THC), the psychoactive compound that produces the ‘high’ in recreational cannabis. All mammals produce endocannabinoids that are involved in a variety of processes, including pain, memory, mood and appetite. Thus in the simplest terms, our bodies are capable of interacting with cannabinoids, and research here is beginning to give some clues as to the possibilities. Pain, multiple sclerosis, Parkinsonism and cancer are all areas of promise – both for palliatives and outright cures. Progress is most likely in areas where cannabinoids show easily demonstrable effects, including the treatment of pain, muscle relaxation, management of nausea, and treatment of anxiety and depression. Longer-term, however, other fields, including the huge realm of cancer, are attracting research interest. A 2007 study by Harvard Medical School gave an early indication of the possibilities, showing some effectiveness with THC in the inhibition of the growth of tumour cells in certain lung cancers.
The move to legalisation in the UK has, in the best British tradition, edged erratically forward as the forces of moral outrage, reason and sentimentality have triumphed in turn. Medical cannabis received an important boost from the outpouring of public support for the plight of seven-year-old Alfie Dingley in 2018. Alfie suffered from a rare and debilitating form of epilepsy. This responded well to a THC-based therapy which the British authorities refused to prescribe or permit to be imported, prompting his family to move to the Netherlands, where it was available. Following a massive campaign, a licence to import the treatment was granted to Alfie’s family, and the then-Home Secretary Sajid Javid announced that doctors would be legally allowed to prescribe medical cannabis from November 2018, although to date only specialists can issue such prescriptions.
In the leisure use category, a typical British fudge is in place. Under the 1971 Misuse of Drugs Act, all drugs are ranked by letter, with penalties for distribution and possession declining with the ranking. At the top is Class A, which includes the metropolitan middle- class favourite, cocaine. Cannabis is currently Class B, having been demoted to C in 2004, then raised back to B in 2008 (against expert advice) by Gordon Brown. In theory, possession of any class B drug can bring up to five years in prison and an unlimited fine. In practice however, police forces have increasingly decided not to pursue charges against recreational users. As a consequence of this the country permits the use of the product, while ensuring that no consistency of quality control is in place, that distribution is in the hands of criminals, and that a potential source of tax revenues is lost.
In the rest of the world, so far only Canada and Uruguay have fully legalised, although other countries such as South Africa and Spain have decriminalised consumption, while commercial distribution generally remains illegal. In the USA, recreational (and medical) cannabis is illegal at the Federal level, but recreational is legal (with varying degrees of regulation) in 11 states, and medical in 33. As a consequence of the Federal illegality, cannabis entrepreneurs have problems with banking and taxation, so this remains very much a cash business.
The market opportunity for cannabis has attracted serious entrepreneurial interest. Estimates of the size of the potential market are vague, but most experts put the annual global medical potential as ultimately above $50bn, with pain management the largest therapeutic area by value. The recreational market is probably somewhat smaller, with estimates suggesting it might be around $30m ten years hence. This, incidentally, is roughly one-tenth of the estimated size of the illegal drug market. As the largest fully legal market, Canada is home to a number of consumer product companies distributing branded products for recreational use. For now, most medical funding comes from venture capitalists, often working in joint ventures with academic institutions. For instance, in 2017 Oxford University partnered with Kingsley Capital to form Oxford Cannabinoid Technologies, which will seek to identify and commercialise therapies based on cannabinoids.
It is likely that the emergence of legal cannabis will follow the pattern identified by Bill Gates, in that we overestimate the rate of change on a two-year horizon, but underestimate it on a ten-year one. Cultural and political suspicions of cannabis remain and in the medical arena the pool of doctors with practical knowledge and experience of cannabis-based therapeutics remains extremely small. As it is, we have almost 50 years of ‘lost’ research time to make up. That and the prospect of a growing array of real solutions to real problems, combined with the failed tactic of criminalising an activity that generates far less harm than the legal alcohol and tobacco industries, means that cannabis use will only grow, and legal obstacles decline.



