
Along with thousands of others, I have watched with increasing anger, sadness and frustration as misinformation has been allowed to spread so freely in the last year, not just on social media but across mainstream media outlets too. I have found myself repeatedly engaging with Covid-19 deniers and lockdown sceptics on social media, trying to answer the same questions and address the same misconceptions over and over again. I have had varying degrees of success, ranging from being thanked for my patience through to being blocked at the point where I mention I have a degree in molecular biology!
Information and statistics are often thrown around by those trying to downplay the pandemic and can sound plausible, making it hard to know what is real and what isn’t. So, I thought I’d bring together the claims and questions I see regularly and debunk/answer them as simply as possible. Hopefully, this will form a useful resource for others wanting to understand the facts behind the pandemic.
“There have only been 388 Covid-19 deaths among the under-60s in the UK.“
This is a truly callous claim. It came from a report in various newspapers stating “388 people aged under 60 with ‘NO underlying health conditions’ have died of Covid-19 in England’s hospitals” in December 2020.
However, the list of pre-existing health conditions covered anything from autism to asthma, learning difficulties to angina, and fractured arms to glaucoma.
To discount the death from Covid-19 of someone who is autistic as a means of trying to minimise the severity of the disease is quite frankly sickening; as is discounting the death of anyone over 60. To date, over 80,000 people have died in the UK as a direct result of Covid-19, all leaving behind sons and daughters, brothers and sisters, friends, partners and loved ones. Discounting their deaths because they had learning difficulties or because they are over 60 is a dangerous path on which to travel.
“Covid-19 only kills people who were about to die anyway.“
This is related to the previous claim and is regularly used to downplay the numbers. There are two very stark pieces of evidence that easily disprove this claim.
First – excess deaths. A five-year average of the number of people who die each week, month or year can be compared to the number of deaths in the same time period this year. The cause of death is irrelevant; it is simply a measure of how many more people died than you would have expected in a normal year. In 2020, around 73,000 more people died than the average of the previous five years. That’s 14 per cent above the average – the highest excess death number we’ve seen in the UK since 1940.
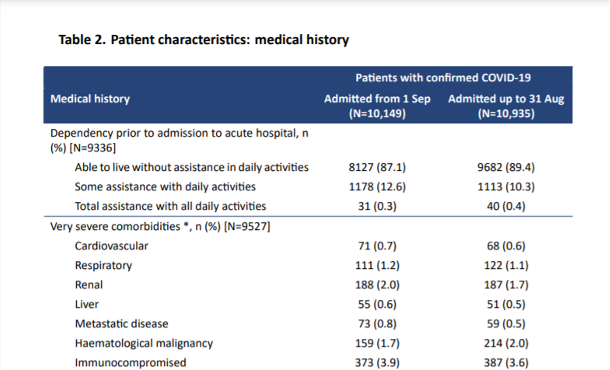
Second – intensive care unit (ICU) statistics. The Intensive Care National Audit and Research Centre (ICNARC) produces a regular report (here) on the characteristics of patients in intensive care in the UK. These are the most severely ill patients, with around 30 per cent not surviving. Of these patients in ICU, nearly 90 per cent were living fully unassisted lives prior to admission, with less than 0.5 per cent needing round-the-clock care. Less than 10 per cent were considered to have severe comorbidities (underlying health factors). These were people living fully active lives before contracting Covid-19.
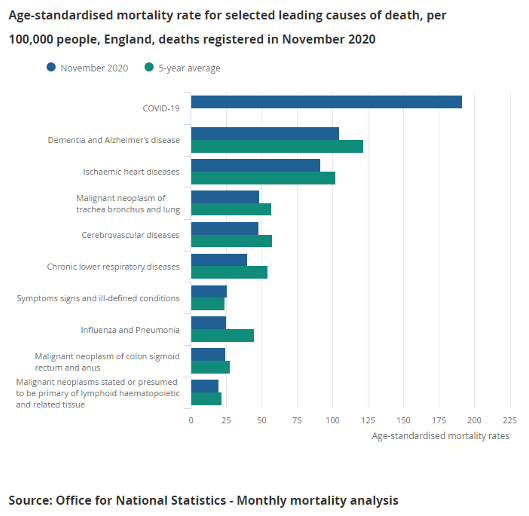
“In September, Covid-19 was the 19th highest cause of death. 19th!! Why are we not addressing the 18 others before it?“
In September, deaths from Covid-19 were low following the initial lockdown and the warm summer months. Unfortunately, that was the calm before the storm. According to the Office for National Statistics (ONS): “The coronavirus (Covid-19) was the leading cause of death in November 2020 for the first time since May 2020 in both England (accounting for 18.1 per cent of all deaths registered in November) and Wales (21.6 per cent of all deaths); looking at all deaths registered in January to November 2020, Covid-19 was the second most common cause of death in England and Wales (after dementia and Alzheimer’s disease).”
And we are still addressing the other causes. But none of them have the infection rates and mortality rates of Covid-19. They continue to be treated (as long as hospitals have capacity), as they have always been.
“Why are there many videos of empty hospitals?“
Because many hospitals have had to close wards to increase their ICU capacity. An empty ward simply shows that staff have had to be deployed elsewhere and so the ward cannot remain open.
[Ed: In addition, Covid-deniers have been posting stock images of empty wards, some of them not even in the UK, to claim that Covid-19 is a hoax.]
“Why are the Nightingale facilities being dismantled and closed?“
Because, unfortunately, they were only ever a nice idea or PR stunt (depending on your viewpoint!). They were simply buildings with beds and some ventilators, but they were never equipped with staff – making them unusable. For a patient to be transferred there they needed to come with staff – which hospitals could not spare.
“Hospitals are always busy in the winter and none of them have reached full capacity yet?“
Yes, hospitals are often busy in the winter, but NHS staff are reporting that they’ve never been hit like this. The capacity figures can be misleading as they are often quoted as a percentage of the available beds. Most ICUs have doubled or tripled their capacity over the last few months, by closing down other departments, theatres, etc and re-deploying staff. So, a hospital that usually has 50 ICU beds may now have 150 beds. If 135 of those beds are full, this is reported as being at 90-per-cent capacity – a figure seen regularly in winter – when actually they are at 270-per-cent capacity compared to normal.
The Financial Times statistician, John Burn-Murdoch has produced a very good animation comparing this winter to previous ones. The numbers for this winter are literally off the scale compared to the last six winters.
“How do we know whether people have died FROM Covid-19 as opposed to just WITH Covid-19?“
There are many claims that people are dying following a positive Covid-19 test from causes unrelated to their Covid-19 infection.
Now, obviously, there will be a tiny number of people for whom that is the case. But the overwhelming majority of people who die within 28 days of getting a positive Covid-19 test are dying as a direct result of contracting Covid-19.
We have multiple sources that show this to be true:
- Excess deaths have mirrored the rise and fall in Covid-19 deaths pretty accurately, suggesting that these excess deaths are the result of people dying from Covid-19. If these people were dying from ‘regular’ causes and just happened to have had a positive Covid-19 test, there would not have been any excess deaths.
- Doctors are well trained in diagnosing disease and are very good at using all the information available to them to make the call on cause of death. When they fill out a death certificate, they write down the event that directly led to death, but they can also write down other contributing factors, including the presence of a positive Covid-19 test and other underlying factors. If a patient dies from cancer, while being positive for Covid-19, the cause will be cancer with Covid-19 mentioned. If a patient undergoing cancer treatment contracts Covid-19 and dies from the effects of Covid-19 (inability to breath, etc), then the cause of death is Covid-19 with cancer mentioned.
- The ONS analyses all these death certificates, looking at the direct cause and the other factors mentioned, and differentiates those who have died WITH and those who have died FROM Covid-19. This data is released every week, and shows that between 80 and 90 per cent of deaths where Covid-19 is mentioned on the death certificate are the direct result of the Covid-19 infection.
“Why are deaths being marked as Covid-19 up to 28 days after a positive test if we only have to isolate for 10–14 days after testing positive?“
Back in the spring, the easiest and quickest way to collate daily data on Covid-19 deaths was to compare anyone who had died with the database of those who had had a positive Covid-19 test. As testing was only being done on people with severe symptoms at that time, it was a reasonable assumption that those who tested positive and then passed away died from Covid-19.
However, by the summer, as fewer people were dying from Covid-19, and more people were ending up on the positive-test list, it became more likely that someone could die from something unrelated to a Covid-19 test that they may have had months before.
A review of the available data showed that 88 per cent of Covid-19 deaths occurred within 28 days of a positive test (96 per cent occurred within 60 days). The 28-day timescale was also being used in other countries for their reporting, so it was chosen as the UK cut-off.
The chance of anyone testing positive for Covid-19 and then dying of something unrelated within four weeks is vanishingly tiny. However, we do know that the 28-day cut-off underestimates Covid-19 deaths.
For those who do not need hospital treatment, the 10–14-day isolation covers the time when they are most infectious and so should stay at home.
“Why, when they have already been caught in August exaggerating Covid-19 death figures, do you not think they’d do it again?“
August was when they made the decision to introduce the 28-day cut-off, which led to a number of deaths being removed from the official statistics. As we know from ONS data based on death certificates, the running total of ‘official’ Covid-19 deaths was already lower than the number of actual Covid-19 deaths. This decision actually made this problem even worse. So, far from ‘being caught exaggerating the figures’, they were making their underestimates even more pronounced.
“In 99.9 per cent of cases, people’s immune systems deal with the virus perfectly well.“
I’ve seen many people trying to claim that over 99.9 per cent of people who catch the virus survive, but, first, the figure is simply not true and, second, dying is not the only adverse outcome.
Of those who contract Covid-19, around 1 per cent will die from it. This varies greatly depending on your age (over-80s have a 15-per-cent chance of dying, with the percentage for under-40s being very low).
However, a further 5 per cent require hospitalisation, and with treatment will survive. These patients would be unlikely to survive without hospital treatment, so the mortality rate increases as hospitals become overrun.
As well as simply looking at death or survival, the long-term health effects of Covid-19 need to be considered. According to the ‘ZOE COVID Symptom Study’: “Long Covid-19 affects around 10 per cent of 18–49-year-olds who become unwell with Covid-19, rising to 22 per cent of over-70s”, which is likely to add an increased burden to our health system and economy for months and years to come.
So, deaths are not the only thing to worry about. But even if they were, a 1-per-cent mortality rate in a highly transmissible disease is very much a reason to take it seriously. 1 per cent of the UK population would be 680,000 deaths …
“People die all the time. It’s a fact of life.“
That’s true, but the sheer number of people who have died in the last 10 months from Covid-19 is hard to imagine. 80,000 people in the UK have died from Covid-19 since February 2020. That is the capacity of the Olympic Stadium.

Since 1900, only two years have seen more than 600,000 deaths in the UK – 1918 (the year of the Global Flu Pandemic, commonly and unfairly known as ‘Spanish’ flu) and 2020.
Conclusion
Covid-19 is real. It is dangerous and needs to be taken seriously. Please follow the rules, everybody!



