Did we try hard enough to “Find the Sick!”? Dr Dan Goylan exposes another Covid mistake.
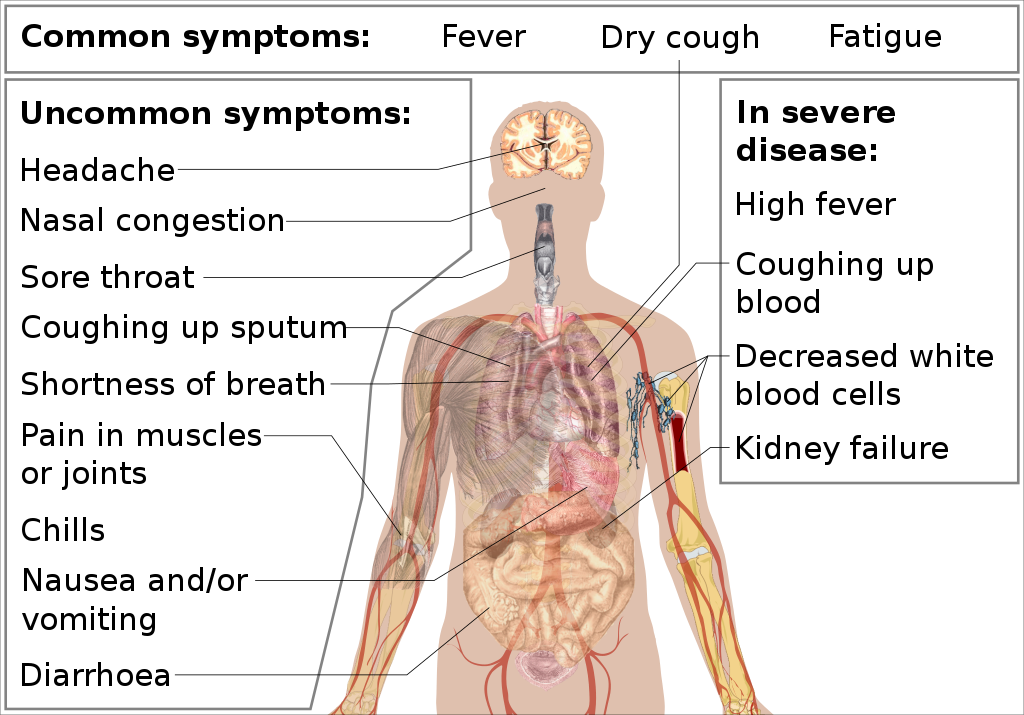
Symptom Profiles:
Why did the UK not include the other common symptoms of Covid for testing and case I.D.?
Does this expose the true motives of the UK’s approach?
By now we have all learned the symptoms of Covid, at least those symptoms that lead to a PCR test in the UK:
1. Fever
2. Cough – “new and persistent”
3. Loss of taste or smell
But most of us are also aware that Covid can present just like a cold or flu or gut symptoms or in other ways.
Even from the start of the pandemic the choice the UK made to narrow the symptoms down seemed very odd. Undoubtably many cases – perhaps the majority – would be missed. This would mean containing the viral spread via Test and Trace would be near impossible.
As time went by…
..evidence grew of just how poor the three symptoms were in catching Covid cases.
The world-famous ISARIC study, analysed many thousands of cases each month, and kept raising concern about the lack of sensitivity of cough, fever and taste/smell issues in picking up Covid.
They also found that many patients could present with non-chest symptoms and still be found to have life-threatening lung disease. Gut symptoms (D&V, abdominal pain) and confusion could be the only presentation of Covid prior to respiratory failure. No cough. No fever. No loss smell.
Yet still the UK did not expand its symptom profile.
It did add in loss of taste and smell in 2020. Thought to be both pathgnomic (quite Covid specific) and linked with poorer outcomes, it made sense to add it.
But why not the others? Is this not accepting more viral spread?
This was raised vocally several times through the pandemic.
A group of more than 140 GPs raised the concern very clearly:
“It is vital to now change the UK covid-19 case definition and test criteria to include coryza and cold, making them consistent with WHO”
https://doi.org/10.1136/bmj.n283
By this point there was no doubt Covid could present like a cold or flu, and most countries were already testing much more broadly.
Yet still, and to this day, the UK policy remains stubbornly limited to these three symptoms.
There are significant consequences both from a public health level and an individual patient risk perspective.
Patients can present with none of the UK approved symptoms and be seriously unwell. Some even present with silent hypoxia. This means treatment is delayed.
Delayed presentation of Covid has been a huge problem for the UK and remains so. In April 2020, average time to admission from symptom onset was over ten days. Even by September this remained at 7 days. (Note Singapore is less than 4 days). Also time to intubation has been revealing…
…over two thirds of patients intubated in 2020 were intubated within the first 24 hours of admission. People were presenting in extremis. Silent hypoxia and lack of UK defined core symptoms are very likely to have contributed to such delays and, sadly, deaths.
Then there is the public health impact. Failing to catch so many cases, allowing people with “head colds” to mix simply increases the spread. Test and trace had little chance, and we were then forced to rely on tougher restrictions. Instead of isolating the sick, the UK…
…isolated everyone!
So, why do it? Why not include all the Covid symptoms?
Test shortages seem unlikely for two years. Too much work seems unlikely given the numbers we eventually tested.
In my view, it is only when you consider it from a herd immunity perspective that it makes sense
Fever can be a worrying symptom. Unremitting fever is a sign of disease progression. So might this pick up some severe cases? Also other things present with fever so it’s important to rule Covid out.
Persistent cough can be a sign of disease progression, too – pneumonitis!
Were the U.K. just trying to detect the severe cases? And therefore let the mild cases spread?
If so, lots of questions about lots of assumptions here. The main one being, could we have prevented long lockdowns had we included all Covid symptoms in case definition?
Whatever the reason, to my mind the failure to adjust symptom profiles indicates a failure to “follow the science” or a stubborn fixation on herd immunity through mass infection. Policy influencing clinical care standards once again?
Originally tweeted by Dr Dan Goyal (@danielgoyal) on 03/03/2022.



