As a retired microbiologist I’ve watched events over the last year with horror and anger. Following the recent excellent Debunking Covid Myths by Emma Monk and the inimitable piece by Femi Oluwole, I want to discuss some grey areas and the significance of new developments, and suggest how we move forward.
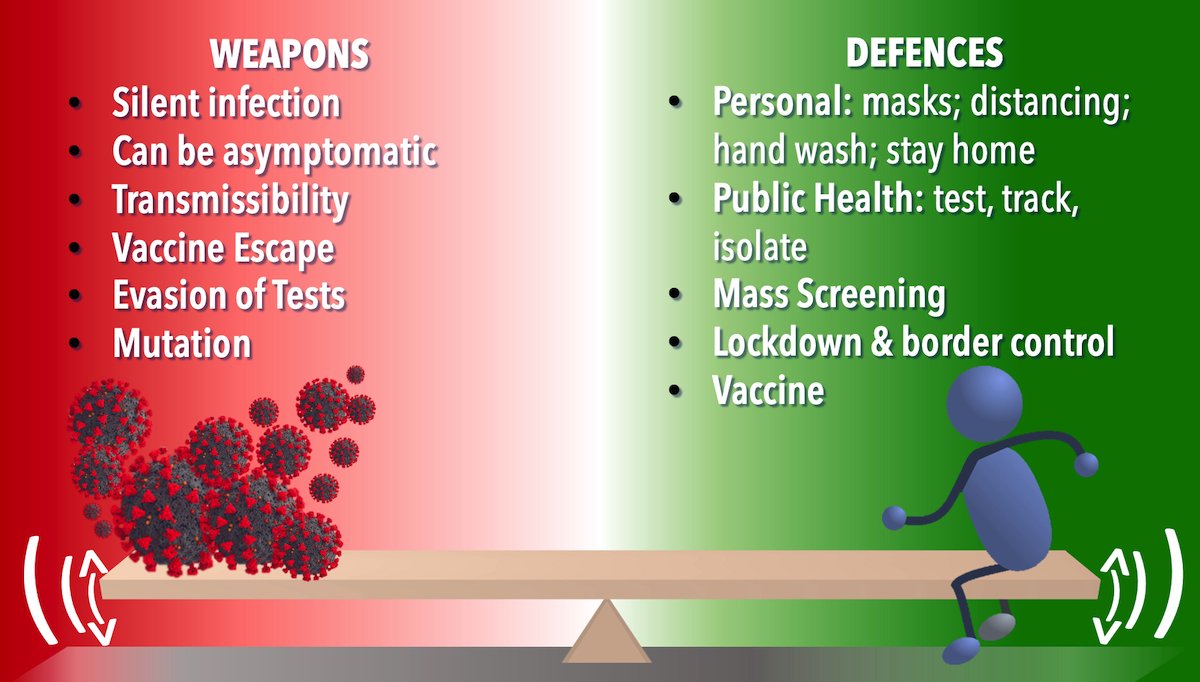
In many ways the war analogy is a bad one for the pandemic. SARS-CoV-2 didn’t choose to infect humans; it lived in a stable relationship with a wild animal. We as humans made the contact and the virus, being ill-adapted to humans, caused illness quite unlike the relative harmony in its natural host. On another level, the analogy is a good one because we have tried various means to keep the virus at bay whilst it counter attacks (albeit without ‘intent’) by evolving through spontaneous mutation and natural selection pressures.
Our defences and its devices interact in a complex way with ups and downs and the outcome is far from clear.
What do the two sides have?
Personal Protection
- Hands, Face Space: a flawed paradigm
Behind the “Hands, Face, Space” mantra is the premise that we can acquire infection by two means – firstly via our hands by touching contaminated objects (known as fomites); and secondly by directly inhaling droplets shed by an infected individual.
Hands
There’s growing evidence that SARS-CoV-2 survival on surfaces is short lived and so it’s probably only significant in instances where an infected person coughs or sneezes on the surface and someone else touches that surface soon after the cough or sneeze (within one to two hours)
The USA’s CDC (Centre for Disease Control) modified its advice in October 2020 to say “touching surfaces is not thought to be a common way that Covid-19 is spread.”
It’s anathema for a microbiologist to decry hand washing but over-reliance on this as a defence against the virus is misguided.
Droplets and aerosols
Droplets are particles shed from the nose and mouth that are large enough to be seen with appropriate lighting. They are regarded as the major vehicle of infection. Crucially they are heavy, so they rapidly fall to the ground – hence our two-metre rule. In addition, wearing even a relatively simple face covering will stop the dispersal of droplets.
By contrast, aerosols are much smaller particles which float in the air. For every droplet we emit, we liberate 1200 aerosols so that we are surrounded by invisible clouds of them. Simple masks will reduce but not eliminate aerosol emissions. Airborne spread by aerosols has been downplayed by official bodies but there is growing evidence for their importance. It is indoors that aerosols are particularly significant as vectors of infection that can spread way beyond two metres, and accumulate and remain in the air for hours. Activities such as singing, shouting or exercising increase aerosol generation and inadequate ventilation allows these to build up.
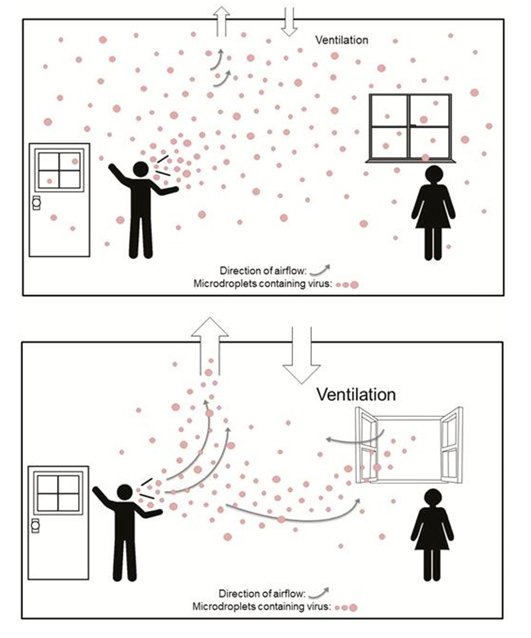
The diagram shows how ventilation mitigates the risk of aerosols but to be effective it needs to be like living in a marquee with open sides. Unfortunately, having all the windows wide open is unlikely to be popular in winter.
Private houses are the obvious setting where aerosol/airborne transmission is significant. However, it can also be relevant in settings such as public transport, restaurants and the workplace. New variants (see below) potentially mean aerosol transmission of infection is even more important.
Although there is information on aerosols and the importance of ventilation in government guidance, it simply hasn’t come through in the overall message. What is more, the guidance implies that wearing a simple face covering will be an effective defence. Could this relaxed guidance possibly relate to the recklessness of the “eat out to help out” summer campaign, the instruction for office workers to return to their offices in the summer and the almost criminal wheeze of giving the virus a Christmas spree when family and friends could meet in their own homes?
All in a day’s work?
Key workers such as health care staff cannot work from home and face a significantly greater risk of infection. In addition, in the first week of the current lockdown, there were 182 workplace related clusters not including hospitals, care homes or schools.
Workplaces may provide ideal conditions for airborne spread with hours spent in a probably inadequately ventilated area with many other staff. The TUC has expressed concern about the paucity of Covid-secure workplace assessments and a trend towards staff being forced back to the workplace, even when work was non-essential or could be done from home
Let’s talk about masks
The intention of the rules is to limit spread of droplets from an infected person. Simple face coverings don’t effectively contain aerosols and offer little protection to wearers. Although there is government guidance, I suspect that few read this and public health messages don’t include practical details. Incorrectly used, masks could cause more harm than good.
Which? did a survey of reusable fabric masks and found huge variations in filtering efficiency. Home-made fabric masks should have at least 2 layers of fabric and should fit well if they are to work.
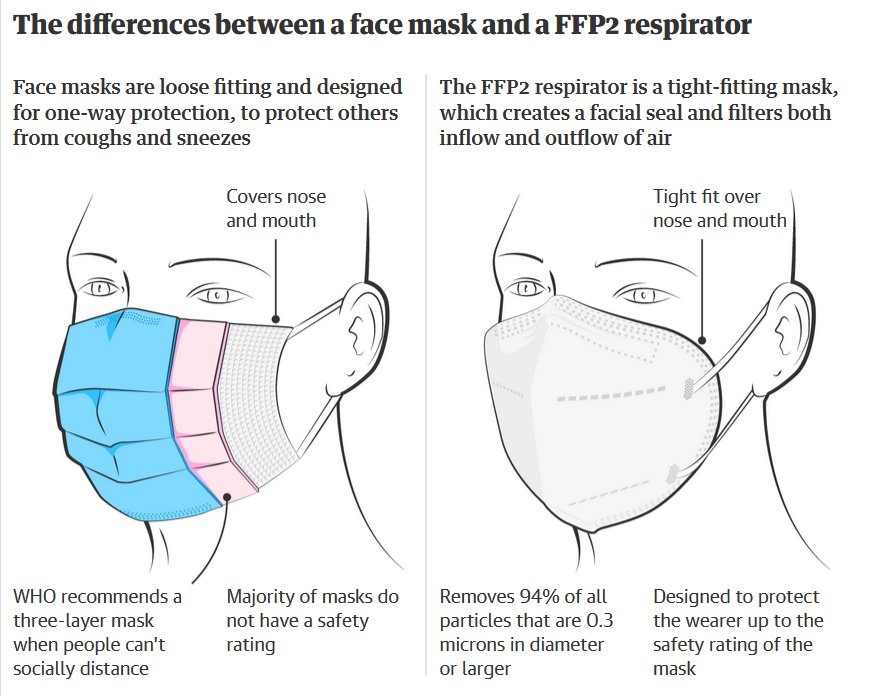
Amid growing concern about increased transmissibility of variants, Austria and Bavaria have mandated the use of so called FFP2 respirators on public transport and in shops.
These will help prevent the escape of aerosols and also provide some protection for wearers. However they are single use, expensive and in short supply. It would be a very big step to require their use in the UK.
2) Common mistakes we all still make
A recent article in the Guardian highlighted aspects of behaviour which even those trying hard to be compliant exhibit from time to time.
These include pushing up to the limits of the guidance rather than making the safest choices, and blindly trusting friends who say they’ve been careful.
National Control Measures
- Test, Trace, Isolate & Support
The Independent Sage Report describes how the testing, contact tracing, isolation and support system should work.
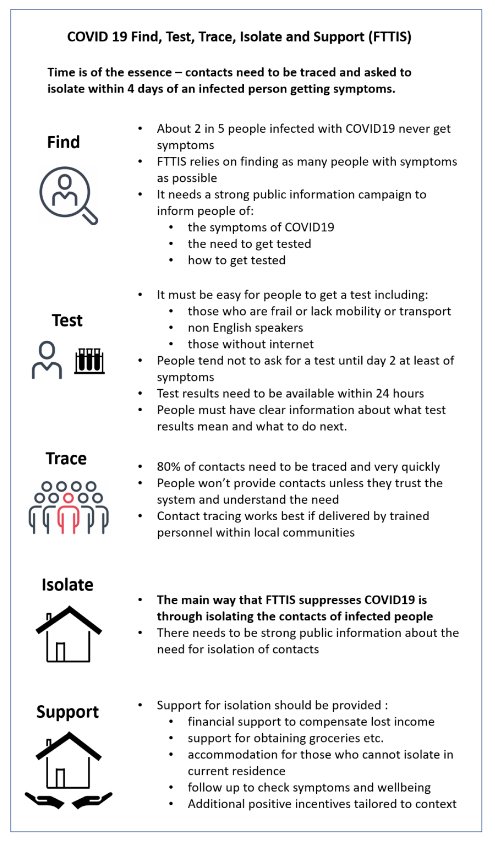
However, the reality is somewhat different:
Testing:
Although testing capacity in Pillar 2 laboratories has improved, the system still fails to achieve a 24hour turnaround time on a reliable basis.
Contact Tracing:
Contact tracing using experienced staff is long established for infections such as tuberculosis and HIV. A combination of tact, persuasiveness and persistence is required to obtain sensitive information, build up trust and ensure that all contacts are identified, contacted and given appropriate advice which they then follow.
The decision to set up “NHS” test and trace using private companies bypassed all this expertise. A Guardian exposé described how young inexperienced staff in huge offices, working alongside telesales firms for gambling websites, ended up doing the job of contact tracing with no real understanding of “the big picture” and how to gain the trust of those to whom they were speaking. In addition, there was huge pressure to skip through the script to get through calls quickly.
The outcomes of Test & Trace have not been encouraging and are some way off the world-beating system promised by the politicians.
Effective contact tracing as done by Public Health staff is time consuming. During the summer of 2020, when rates were relatively low, it would have been possible to chase down infection and stop transmission. This opportunity was wasted and now, with the massive infection rates we have seen in recent weeks, it would be extremely difficult for contact tracing to interrupt community transmission to any significant degree.
Isolation & Support
Although this is a key part of control it seems it was only ever an afterthought for ‘NHS’ Test & Trace.The ability to self-isolate depends on having the space and resources to do so. Survey data from the UK suggest that fewer than one in five people can adhere to isolation protocols. Although willingness to self-isolate was high across all respondents, the self-reported ability to isolate was three times lower among those earning less than £20, 000 a year or who had less than £100 saved. Lost wages are the primary reason for not following isolation guidelines. At the same time this is the group most likely to be exposed to infection through occupation and therefore most often subject to self-isolation requests.
Even now, the majority of people have been refused a discretionary self-isolation payment, while statutory sick pay is a paltry £95.85 a week. By contrast, Finland and Norway offer 100% and 80% of income to people who are self-isolating. The result of the UK’s inadequate support is that many who have tested positive have ended up going into work and infecting others.
2) Mass Screening – key intervention or handing cash to chums?
You’ll have heard of Johnson’s proposed “Operation Moonshot”. The idea is predicated on asymptomatic infections being a hidden driver of the pandemic. In the 24 to 48 hours before symptoms develop, individuals are shedding large amounts of virus and can be highly infectious. Part of the urgency of contact tracing is to get such individuals to self-isolate before they transmit infection.
However, only around 20% of individuals remain asymptomatic throughout.
There has been much debate about how significant these individuals are in spread of the virus. Although likely to circulate unrestricted in the community (because they are unaware they have the virus), they do actually appear to be less infectious. Mass screening could not be compulsory. Many of those at increased risk of infection through their occupation such as taxi drivers, cleaners and retail staff would be reluctant to take a test because of the loss of income they might incur. A pilot study of screening was done in Liverpool with Lateral Flow tests because they are quick and, like a pregnancy test, don’t require laboratory processing.
What is more, use of the rapid but insensitive Lateral Flow Test may give negative results which provides recipients with the false reassurance of a ‘Covid-free passport’. In September 2020, SAGE recommended that “Prioritising rapid testing of symptomatic people is likely to have a greater impact on identifying positive cases and reducing transmission than frequent testing of asymptomatic people in an outbreak area.” Did the government’s enthusiasm for mass testing with the unreliable Lateral Flow test relate to a misguided belief that it could relax control measures earlier as a consequence?
3) Vaccines: are they a weapon in the war?
The progress with coronavirus vaccines is truly astonishing with 3 vaccines now in use in the UK. The first priority, as determined by the Joint Committee on Vaccines and Immunisation (JCVI), was to target the highest risk groups for severe disease and thereby limit hospital admissions and deaths.
In terms of fighting the war against SARS-CoV-2 what we don’t know is whether immunisation will just protect against symptomatic illness or prevent infection altogether. There is some limited but encouraging data, but more information is required. Certainly, the expectation would be that if vaccinees were to be infected they would be less infectious, so vaccines could help interrupt transmission. It is very encouraging that in UK trials of the Oxford Astra Zeneca vaccine, the immunised group yielded 67% fewer positive Covid-19 swabs than the placebo group. This could be highly significant.
When the vulnerable have been immunised can we relax?
The answer to this is an emphatic no. At that stage, the majority of unimmunised will still be susceptible. Without controls the virus would circulate freely with the danger of
1) infecting vulnerable groups who haven’t responded to the vaccine;
2) encouraging emergence of vaccine escape mutants
3) Even in 18-65-year-olds infection can be severe (Yes, Prime Minister!) and Long-Covid can affect 10 per cent in this age group.
Worryingly, studies show that 40 per cent of people say they will either stop following rules or relax their level of compliance after immunisation.
We’re only safe when we’re all safe.
Vaccine nationalism is the almost inevitable consequence of a limited supply. However, the reality is that to prevent vaccine-resistant mutants taking over and nullifying our vaccine efforts global vaccination is required.
Jeremy Farrar a member of SAGE has warned that immunising “a lot of people in a few countries, leaving the virus unchecked in large parts of the world, will lead to more variants emerging”.
Covax is a WHO supported voluntary arrangement that enables countries to pool their resources and risk by collectively investing in vaccine candidates, while developing the political and logistical infrastructure needed for vaccine distribution. Most importantly, Covax ensures that vaccines financed through the initiative will be allocated in a transparent and coordinated manner. How well this works in practice remains to be seen. The UK has committed £548m in aid to help supply vaccines to 92 countries. It’s a sobering thought that it’s likely to be 2023 or 2024 before anything like global vaccine cover is achieved.
What about the delayed second dose?
I’m clear that the decision of the Joint Committee on Vaccines and Immunisation (JCVI) is correct. Given the severely limited vaccine supplies at present, the greatest benefit for the population is achieved by allowing more people to receive a single dose as soon as possible. If you have 200,000 doses and give 100,000 people two doses then you’ll protect 95,000 people (based on 95% efficacy). By contrast, if you give 200,000 people one dose even with a pessimistic assumption of 60% efficacy, 120,000 will be protected. In addition, the efficacy data for one dose are skewed by infections arising in the first 21 days after vaccine when protection isn’t expected anyway. Everyone will, of course, get a second dose by 12 weeks.
Does the Oxford Astra Zeneca vaccine work in the elderly?
This controversy was started by the decision of the Robert Koch Institute not to recommend its use in those over 65. The trials were conducted in UK, South Africa and Brazil. Older cohorts were largely in the UK and were recruited late in the process. Because there was relatively little Covid-19 in the UK at the time of the study there were insufficient cases of Covid-19 illness (two) in the older age group to establish efficacy – ie whether there was a significant difference between cases and controls. However, the antibody response in over-65s was as good as that in younger cohorts, strongly suggesting that vaccine will protect against symptomatic infection in this age group.
The European Medicines Agency has approved the AstraZeneca vaccine for use in the EU on people over 18, without an upper age limit. I (aged 70) have no preference as to which vaccine I receive.
4) Control of borders and quarantine of entrants
This is an area in which Britain has been woefully inactive. Even when controls have been in place at arrival points, travellers have been allowed to travel onwards by public transport and potentially infect others. Follow up to confirm adherence to quarantine has been minimal. This is finally being addressed.
“Weapons” in the Virus Armoury – Variants
The 100 million SARS-CoV-2 human infections worldwide have offered great scope for mutation and inevitably some of these will convey survival advantages for the virus. Surveillance is undertaken by genetic sequencing of viruses detected in cases.
To date three variants of concern (VOCs) have been identified globally. The naming of these has not been officially agreed but they are: UK variant B.1.1.7, South Africa Variant B.1.351 and Brazil variant P1. Genetic sequencing is carried out with wide differences in frequency in different countries so there may be many other significant variants out there that have not yet been detected.
Three different effects of mutations have been identified.
- Severity of Disease
There are preliminary data to suggest that infection with B.1.1.7 variant is associated with an increased risk of death.
- Transmissibility
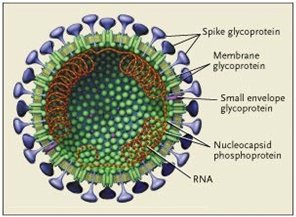
All 3 VOCs have a mutation (N501Y) affecting the spike glycoprotein so that the virus binds more effectively to the receptor on human cells, increasing transmissibility by up to 70%.
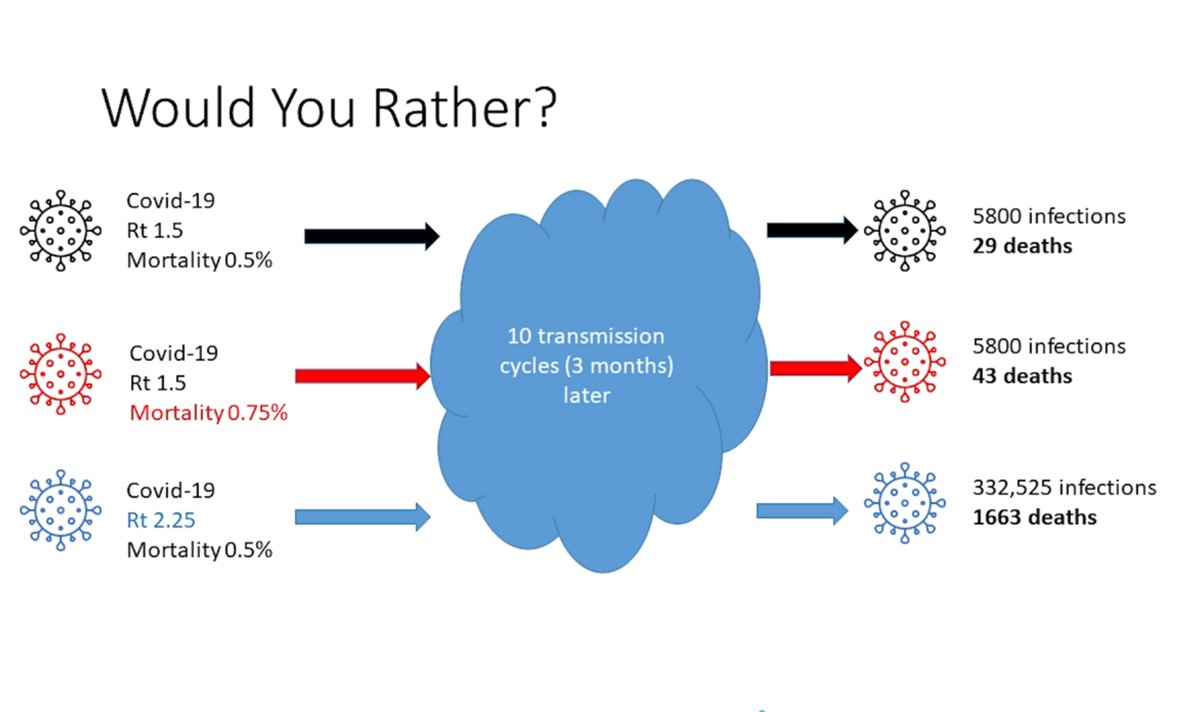
To understand the significance of this one must recall that the virus can cycle through humans in around 6 days; so, like insanely fast compound interest, in just three months the number of infections can mushroom alarmingly and, correspondingly, the number of deaths as shown by the diagram.
Increased transmissibility is much more worrying than increased risk of death.
As an example, B.1.1.7 was first detected in Kent, but within weeks it had spread to all regions and accounted for 60% of cases in England.
It has now been detected in 64 countries. The Brazil strain spread rapidly and by late December 2020 accounted for 42% of strains in Manaus, a large city in the Amazon region where SARS-CoV-2 is rampant.
- Evasion of vaccine or vaccine-induced immunity
Both the South Africa and the Brazil variants have the E484K spike protein mutation that in lab tests suggest the virus is less effectively neutralised by antibodies compared with conventional strains. As a consequence, current vaccines may be less effective. Clinical trials of the Novavax and Johnson & Johnson candidate vaccines were said to be less effective in South Africa, compared to the UK or USA. This is thought to be due to a high prevalence of virus carrying this E484K mutation
The South Africa variant has been reported in at least 26 countries and more than almost 100 cases have been seen in the UK. Worryingly it has now been detected in 11 cases with no history of foreign travel.
A huge Public Health effort is underway in 8 different parts of the country to try to find any other cases and control spread.
It now emerges that a B.1.1.7 variant and an original Wuhan strain have been identified in the UK which have the E484K mutation in addition to the N501Y transmissibility mutation.
Widespread immunisation will start to exert selective pressure on the virus and favour other mutations associated with reduced sensitivity to vaccine-induced and natural immunity.
Significance of variants of concern
VOCs could be a game changer and highlight the importance of having a secure system of quarantine for those entering the country and an effective ongoing test, trace and isolate regime. Although vaccine manufacturers can respond to vaccine escape by appropriate editing, the practicalities of having to replace vaccines in short order are enormous. “These won’t be the last variants we’ll see. But if we get infection rates to as close to zero as possible, we’ll reduce the risk of future mutations that can find chinks in our immunity armour”.
Worryingly, on 3 February Tory peer Dido Harding, who is in charge of the UK Government’s National Institute for Health Protection told a shocked Commons science and technology committee that none of her people were able to predict virus mutation or the new variant.
What should we do now?
As an individual:
- Take up the offer of vaccine.
- Don’t think you can abandon Covid precautions when you’re immunised. They’ll continue to be important to protect both you and others.
- Make sure you have appropriate masks and that you use them as per guidance.
- Don’t obsess about surface decontamination and excessive hand washing.
- Be aware of the implications of aerosol/airbornespread.
- Think about what’s safe rather than what’s allowed, especially regarding indoor spaces.
- Take a vitamin D supplement and look after your general health.
Nationally
I fear Johnson will be increasingly hostage to his own MPs in the guise of the ill-named Coronavirus Recovery Group and yet again sabotage our progress out of the pandemic by prematurely relaxing controls. We need:
- Intense and effective campaigns to combat fake news and anti-vaxx conspiracies
- Improved testing turnaround times with results in 24h
- To introduce properly-conducted, locally-based contact tracing
- To provide appropriate support for those needing to quarantine or self-isolate
- To control of our borders with proper follow up of entrants
- A continuation of control measures even when vulnerable groups immunise
- To keep lockdown measures stringent until community infection numbers are very low to give contact tracing a chance to work
- To collaborate on achieving global immunisation
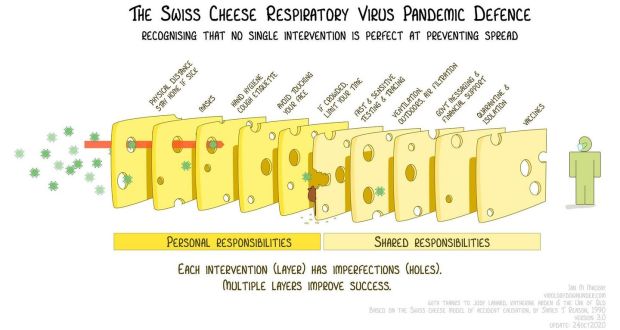
In conclusion and this is a bit cheesy …
It should be clear that there is no magic bullet in the war against the SARS-CoV-2 pandemic. The only hope we have is to implement a whole series of control measures with a high level of efficacy both at a personal and national level. This is known as the Swiss Cheese model as shown in the graphic.